


What is a stepped-wedge cluster randomised trial?
A stepped wedge cluster randomised trial (SW-CRT) is a type of CRT where clusters are randomised to sequences. All or most clusters begin the trial receiving the control condition. During the trial, each sequence switches to the intervention condition at a different time so that, by the end of the trial, all or most of the clusters are receiving the intervention condition. No clusters switch from intervention to control at any time.
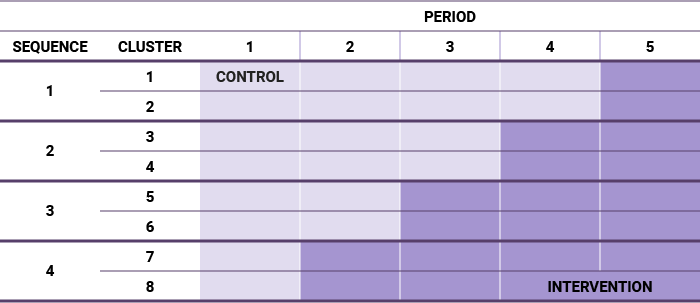
A schematic of a typical SW-CRT (in this case with eight clusters, four sequences, and five steps) looks like the example below.
A related design is the cluster crossover trial. SW-CRTs are a modification of the crossover design. In a cluster crossover trial, clusters are randomised to two sequences. Most cluster crossover trials have two periods only. In one sequence, clusters receive the control condition followed by the intervention. In the other sequence, clusters receive the intervention condition followed by the control. Thus, SW-CRTs are essentially a one-way crossover trial. On this website, we focus on parallel CRTs and SW-CRT, but have included some references for cluster crossover trials in the SW-CRT resources pages.
Cluster and SW-CRT overviews
The following are well-known textbooks and journal articles on cluster and SW-CRTs:
-
Hooper, R. Key concepts in clinical epidemiology: Stepped wedge trials. Journal of Clinical Epidemiology. 2021; 137: p. 159-162.
-
Hayes RJ, Moulton LH. Cluster randomised trials. Boca Raton: CRC Press; 2017
-
Hughes JP, Granston TS, Heagerty PJ. Current issues in the design and analysis of stepped wedge trials. Contemporary Clinical Trials.2015;45:55-60
-
Hargreaves JR, Copas AJ, Beard E, Osrin D, Lewis JJ, Davey C, et al. Five questions to consider before conducting a stepped wedge trial. Trials. 2015;16(1):350
-
Hemming K, Haines TP, Chilton PJ, Girling AJ, Lilford RJ. The stepped wedge cluster randomised trial: rationale, design, analysis, and reporting. British Medical Journal. 2015;350:h391
-
Campbell MJ, Walters SJ. How to Design, Analyse and Report Cluster Randomised Trials in Medicine and Health Related Research. Chichester, West Sussex: John Wiley & Sons; 2014
-
Eldridge S, Kerry S. A Practical Guide to Cluster Randomised Trials in Health Services Research. Chichester, West Sussex: John Wiley & Sons; 2012
Example SW-CRTs
Like with parallel CRTs, SW-CRTs are used in a range of settings, as demonstrated by the examples below:
SW-CRT examples
Health treatment and prevention programs
-
Durovni B, Saraceni V, Moulton LH, Pacheco AG, Cavalcante SC, King BS, et al. Effect of improved tuberculosis screening and isoniazid preventive therapy on incidence of tuberculosis and death in patients with HIV in clinics in Rio de Janeiro, Brazil: a stepped wedge, cluster-randomised trial. The Lancet Infectious Diseases.2013;13(10):852-8
-
Gruber JS, Reygadas F, Arnold BF, Ray I, Nelson K, Colford JM. A Stepped Wedge, Cluster-Randomized Trial of a Household UV-Disinfection and Safe Storage Drinking Water Intervention in Rural Baja California Sur, Mexico. The American Journal of Tropical Medicine and Hygiene. 2013;89(2):238-45
-
Priestley G, Watson W, Rashidian A, Mozley C, Russell D, Wilson J, et al. Introducing Critical Care Outreach: a ward-randomised trial of phased introduction in a general hospital. Intensive Care Medicine. 2004;30(7):1398-404
-
Solomon E, Rees T, Ukoumunne OC, Metcalf B, Hillsdon M. The Devon Active Villages Evaluation (DAVE) trial of a community-level physical activity intervention in rural south-west England: a stepped wedge cluster randomised controlled trial. International Journal of Behavioral Nutrition and Physical Activity. 2014;11(1):94
-
Golden MR, Kerani RP, Stenger M, Hughes JP, Aubin M, Malinski C, et al. Uptake and population-level impact of expedited partner therapy (EPT) on Chlamydia trachomatis and Neisseria gonorrhoeae: the Washington State community-level randomized trial of EPT. PLOS medicine. 2015;12(1):e1001777
Vaccination programs
-
Gambia Hepatitis Study Group. The Gambia Hepatitis Intervention Study. Cancer Research. 1987;47(21):5782-7
Behavioural interventions
-
Pearson DAS, McDougall C, Kanaan M, Torgerson DJ, Bowles RA. Evaluation of the Citizenship Evidence-Based Probation Supervision Program Using a Stepped Wedge Cluster Randomized Controlled Trial. Crime & Delinquency. 2016;62(7):899-924
School-based interventions
-
Mhurchu CN, Gorton D, Turley M, Jiang Y, Michie J, Maddison R, et al. Effects of a free school breakfast programme on children’s attendance, academic achievement and short-term hunger: results from a stepped-wedge, cluster randomised controlled trial. Journal of Epidemiology and Community Health. 2013;67(3):257-64
Why do a SW-CRT?
SW-CRTs have become popular in the last few years. The reasons for randomising clusters are the same as described in why do a CRT? The section below gives an overview of the reasons for performing a SW-CRT. There is disagreement about the validity of some reasons given, as discussed below:
-
Logistical reasons: Some researchers say that it is easier to implement the intervention in an SW-CRT because the intervention is only rolled out to a few clusters at one time. However, some trialists have found it difficult to manage the growing burden of maintaining the intervention in all clusters towards the end of the trial. A parallel CRT only requires maintenance of the intervention in half of all clusters, and can also incorporate a staggered roll out if necessary. In fact, in health services research staggered rollouts in cluster randomised trials are extremely common.
-
Recruitment of clusters: Researchers have found it easier to recruit clusters when they are giving the intervention to all clusters. Other designs can also fulfil this need, for example a waitlist design where control clusters are given the intervention after the trial has ended.
-
Ethics: Some researchers feel like it is a more ethical design when the intervention is expected to be beneficial. However, some have disputed the ethics of with-holding the intervention from clusters randomised to receive the intervention later in such situations.
-
Utilising the rollout of an intervention that is happening anyway: Some SW-CRTs are done as a means of evaluating an intervention as it is being implemented.
For more on the debate about why to do a SW-CRT, see the following papers:
Why do a SW-CRT?
-
Prost A, Binik A, Abubakar I, Roy A, De Allegri M, Mouchoux C, et al. Logistic, ethical, and political dimensions of stepped wedge trials: critical review and case studies. Trials. 2015;16(1):351
-
Kotz D, Spigt M, Arts ICW, Crutzen R, Viechtbauer W. Use of the stepped wedge design cannot be recommended: A critical appraisal and comparison with the classic cluster randomized controlled trial design. Journal of Clinical Epidemiology. 2012;65(12):1249-52
-
Doussau A, Grady C. Deciphering assumptions about stepped wedge designs: the case of Ebola vaccine research. Journal of Medical Ethics. 2016;42(12):797-804
-
Zhan Z, van den Heuvel ER, Doornbos PM, Burger H, Verberne CJ, Wiggers T, et al. Strengths and weaknesses of a stepped wedge cluster randomized design: its application in a colorectal cancer follow-up study. Journal of Clinical Epidemiology. 2014;67(4):454-61
-
Mdege ND, Man M-S, Taylor CA, Torgerson DJ. Systematic review of stepped wedge cluster randomized trials shows that design is particularly used to evaluate interventions during routine implementation. Journal of Clinical Epidemiology.2011;64(9):936-48
Correlation in SW-CRTs
In SW-CRTs observations are not independent of one another. There are two types of correlation to account for in the design and analysis:
-
Intracluster correlation: As with CRTs, observations in the same cluster will be more similar to one another than observations in different clusters. In a SW-CRT, this is the correlation of observations in the same cluster at the same time.
-
Correlations over time within clusters: Unlike a CRT, in a SW-CRT we can get information about the effect of the intervention by comparing observations from the periods that a cluster is in the control condition to observations from periods that the cluster is in the intervention condition. Because of this, we need to account for how similar observations are over time within each cluster.
In general, we would expect observations collected in the same period to be more similar (more correlated) than observations collected in different periods. The correlation between observations in the same cluster but from different periods is sometimes called the inter-period correlation.
Designs with more than two periods may have different inter-period correlations for different pairs of periods. An example of this is autocorrelated data, where observations from periods closer in time are more correlated than observations from periods further apart in time.
Types of design
The schematic above shows a typical SW-CRT, but there are many variations of this design depending on the number of sequences, clusters, periods, and whether different individuals are observed in each period (a repeated cross-section design), or the same individuals are observed over time (a cohort design). Some designs do not collect observations from all clusters in all periods, for example some trials include transition periods, during which the intervention is embedded into the cluster and the cluster is considered neither exposed nor unexposed. See our resources for designing SW-CRTs for more on this.